

Which Of The Following Is Not True Regarding Hospital Emergency Services.
Disquisitional Admission Hospital is a designation given to eligible rural hospitals by the Centers for Medicare & Medicaid Services (CMS). Congress created the Critical Admission Hospital (CAH) designation through the Balanced Budget Act of 1997 (Public Law 105-33) in response to over 400 rural hospital closures during the 1980s and early 1990s. Since its creation, Congress has amended the CAH designation and related program requirements several times through boosted legislation.
The CAH designation is designed to reduce the financial vulnerability of rural hospitals and ameliorate admission to healthcare by keeping essential services in rural communities. To accomplish this goal, CAHs receive sure benefits, such every bit cost-based reimbursement for Medicare services. (encounter What are the benefits of CAH status?)
Eligible hospitals must see the following weather to obtain CAH designation:
- Have 25 or fewer acute intendance inpatient beds
- Be located more than 35 miles from another hospital (exceptions may apply – encounter What are the location requirements for CAH condition?)
- Maintain an annual average length of stay of 96 hours or less for acute intendance patients
- Provide 24/7 emergency care services
Congress besides created the Medicare Rural Hospital Flexibility Plan (Flex Program) in the Counterbalanced Budget Deed of 1997 to support new and existing CAHs.
This guide provides resources concerning the post-obit CAH-related areas:
- Payment/reimbursement and financial data
- Regulations and data regarding CAH status and the Flex Program
- Key organizations in the field
- Funding opportunities
- Challenges to operation
Frequently Asked Questions
- What are the benefits of CAH condition?
- How does Medicaid reimburse CAHs?
- Are all the benefits of CAH condition available in every state?
- What types of facilities are eligible for CAH status?
- What are the location requirements for CAH status?
- How many CAHs are there and where are they located?
- What are the quality balls and quality improvement options for CAHs?
- What is the Medicare Rural Infirmary Flexibility Program and how is it related to the CAH programme?
- Where can I find CAH comparative information?
- Can a CAH own some other healthcare facility?
- Tin can a CAH add an off-campus, provider-based clinic that does not meet the CAH distance requirements?
- What are the requirements for relocating an existing CAH under the Necessary Provider replacement rules?
- Is there a limit on the length of stay for patients at CAHs?
- How many beds are immune?
- What is a swing bed?
- What emergency services are CAHs required to provide? What are staffing requirements for emergency services?
- What kinds of agreements does a CAH demand to have with an acute care infirmary?
- Where tin I find examples of CAH network agreements, tools, and other materials?
- How exercise staffing and other requirements differ for CAHs, compared to general acute care hospitals?
- Are CAHs eligible for the 340B program?
- What sources of capital letter funding exist for CAHs?
- What is the CAH survey process?
- What legislation has affected the Critical Access Infirmary program?
- What are Rural Emergency Hospitals?
- Who tin answer questions about CAH condition or reimbursement bug?
What are the benefits of CAH status?
CAH status includes the following benefits:
- Price-based reimbursement from Medicare. As of January ane, 2004, CAHs are eligible for allowable price plus i% reimbursement. Nonetheless, equally of Apr 1, 2013, CAH reimbursement is subject area to a two% reduction due to sequestration. In some states, CAHs may as well receive cost-based reimbursement from Medicaid.
- Flexible staffing and services, to the extent permitted under country licensure laws.
- Capital improvement costs included in commanded costs for determining Medicare reimbursement.
- Admission to Flex Programme educational resources, technical assistance, and/or grants.
For more information about CAH reimbursement and payment benefits, encounter the Medicare Learning Network: Critical Access Infirmary booklet from CMS, the Pocket-size Rural Infirmary and Clinic Finance 101 manual from the Technical Assist and Services Centre (TASC), or Medicare Payment Basics: Critical Access Hospitals Payment Organization from the Medicare Payment Advisory Commission (MedPAC).
Critical Admission Hospital (CAH) status does not guarantee a better financial state of affairs. Some hospitals will find the cost-based reimbursement advantageous, and some volition not. Each infirmary must perform its own financial analysis to determine if being a Prospective Payment System (PPS) hospital or a CAH would result in a amend fiscal return. For financially distressed hospitals, even if CAH condition leads to increased reimbursement, it may not put the hospital in the black. In fact, some hospitals take closed fifty-fifty after converting to CAH status. The Flex Monitoring Team releases an almanac CAH Financial Indicators Report that can exist helpful in agreement financial operation of CAHs.
CAH status should be considered or maintained only if information technology is advisable for the community demand and hospital service area. In particular, consideration should be given to the bed limit for CAHs and potential service lines and whether they are sufficient to meet community need.
CAH status does not necessarily mean fewer services are offered compared to other facilities. Services offered by a CAH should exist aimed to meet the customs'southward unique needs. Therefore, the number and blazon of services offered in one community may be unlike than in another community. A CAH tin utilize a Community Wellness Needs Assessment (CHNA) to guide its review of electric current and future services needs.
For information about payment methods, eligibility criteria, and financial functioning, run across Medicare Payment for Rural or Geographically Isolated Hospitals and 2016-18 Profitability of Urban and Rural Hospitals past Medicare Payment Classification, which compare the following designations:
- Critical Access Hospital (CAH)
- Sole Community Hospital (SCH)
- Medicare-Dependent Hospital (MDH)
- Rural Referral Center (RRC)
How does Medicaid reimburse CAHs?
Each state determines how it will reimburse CAHs for services through Medicaid. Several states utilize some form of cost-based reimbursement for CAHs, while other states follow a prospective payment arrangement (PPS). Additionally, variation may exist between inpatient and outpatient payment policies.
The Medicaid and Fleck Payment and Access Commission (MACPAC) compiled each state'south Medicaid payment policies for inpatient and outpatient services.
- State Medicaid Payment Policies for Outpatient Hospital Services (July 2016)
Land-specific payment details for CAHs are listed in row 28. - State Medicaid Payment Policies for Inpatient Hospital Services (December 2018)
Country-specific payment details for CAHs are listed in row 17.
For additional information virtually your state's payment policies, consult your State Rural Hospital Flexibility Program Contact.
Are all the benefits of CAH status bachelor in every state?
No. Some states license CAHs under the same licensure rules as other hospitals, and CAHs must comply with those licensure rules. If those rules are stricter than the CAH CoP, the CAH is unable to benefit from the more than flexible Medicare Conditions of Participation (CoP) for CAHs and the related cost savings. In addition, v states — Connecticut, Delaware, Maryland, New Jersey, and Rhode Isle — exercise not have any hospitals with CAH status, and therefore do not participate in the Flex Plan.
What types of facilities are eligible for CAH status?
Facilities applying to get Disquisitional Access Hospitals must be currently participating in the Medicare plan and have a current license as an astute intendance infirmary. Hospitals closed later on November 29, 1989, and hospitals that accept downsized to wellness dispensary or health center status may too authorize for CAH condition if they come across all of the CAH Conditions of Participation.
What are the location requirements for CAH condition?
Critical Access Hospitals must exist located in rural areas and must meet one of the following criteria:
- Exist more than a 35-mile drive from another infirmary, or
- Be more than a 15-mile drive from another hospital in an expanse with mountainous terrain or only secondary roads.
CAHs designated by their state as a Necessary Provider prior to January 1, 2006, are exempt from these distance requirements. See the Centers for Medicare & Medicaid Services' Description of Disquisitional Access Infirmary (CAH) Rural Condition, Location and Distance Requirements and Critical Access Infirmary (CAH) Recertification Checklist for Evaluation of Compliance with the Location and Altitude Requirements for definitions.
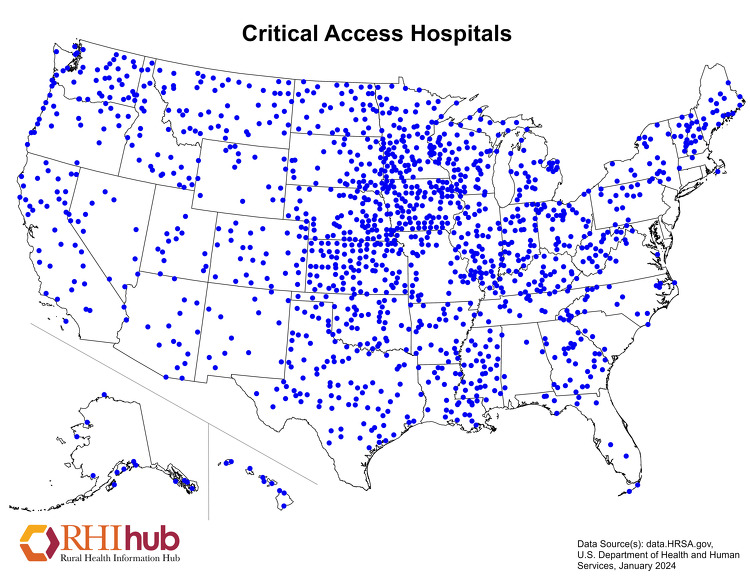
How many CAHs are in that location and where are they located?
The Flex Monitoring Squad maintains a list of Critical Admission Hospitals, which includes the hospital proper noun, city, state, zip code, and constructive date of CAH status.
As of July 16, 2021, at that place are one,353 CAHs located throughout the U.s.a..
The following map shows the locations of Disquisitional Access Hospitals across the United States. Country-level healthcare facility maps are besides bachelor.
What are the quality assurance and quality improvement options for CAHs?
Critical Access Hospitals (CAHs) must have and maintain quality assurance arrangements with at least one of the following:
- One other CAH or hospital that is part of the network
- I quality improvement organization (QIO) or equivalent entity
- I other appropriate and qualified entity as identified in the state's rural health care plan, such as an accrediting trunk.
In add-on to quality balls, quality comeback is important to CAHs. The Medicare Beneficiary Quality Improvement Project (MBQIP), under the Medicare Rural Hospital Flexibility (Flex) Plan, aims to improve quality of care in CAHs by encouraging self-reported quality data, which are analyzed and used to inform activities at the facility. The Flex Monitoring Team'due south MBQIP Quality Measure Trends, 2011-2016 shows CAH operation trends and MBQIP reporting rates during that period. According to the May 2019 MBQIP Monthly, 99% of CAHs in the U.S. written report on at least one domain and 93% reported quality measures in at least iii domains in 2018. Any CAH wanting to receive benefits or services from the land's Flex Program funding must participate in MBQIP and meet the minimum reporting requirements (or submit a waiver if necessary). The National Rural Health Resources Middle also provides resources for Land Flex Programs and providers regarding MBQIP, including Flex Eligibility Criteria for MBQIP Participation and Waiver Templates.
What is the Medicare Rural Infirmary Flexibility Plan and how is it related to the CAH program?
The Medicare Rural Infirmary Flexibility Programme (Flex Program) was created by the Balanced Budget Act of 1997 and is administered through the Federal Office of Rural Health Policy. The Flex Program encourages states to take a holistic approach to strengthening rural healthcare with a focus on Critical Access Hospitals (CAHs) and their Rural Health Clinics, rural emergency medical services (EMS), and rural communities. The Flex Plan provides federal cooperative agreements to eligible states to assistance them achieve their strategic goals, specially in the following areas for Fiscal Years 2019-2023:
- CAH quality improvement (required)
- CAH operational and financial improvement (required)
- Population wellness improvement (optional)
- Rural emergency medical services (Ems) improvement (optional)
- Innovative model development (optional)
- Critical Admission Hospital designation (required if requested)
Specific goals within each priority area are updated for each program cycle to best reflect the needs of CAHs.
The Federal Role of Rural Health Policy also awarded supplemental funding to eight State Flex Programs to conduct demonstration projects to build an evidence base for rural Ems related to quality metrics and sustainable rural Ems models. Implementation of Flex EMS Supplemental Funding Projects: Year One Activities provides an overview of the implementation of the outset twelvemonth of these efforts, which spanned September 2019 to August 2020.
National infrastructure to back up the Flex Program includes:
- Federal Role of Rural Wellness Policy (FORHP) – Administers the Flex Program and its associated grants to states. Located within the Wellness Resources and Services Assistants (HRSA).
- Technical Help and Services Centre (TASC) – Provides information and technical assistance to State Flex Programs and Critical Access Hospitals. Located at the National Rural Health Resources Center.
- Flex Monitoring Team – Conducts research and collects data on CAHs, evaluates the impact of the Flex Plan, and maintains the list of CAH locations beyond the land. Also operates and maintains the Disquisitional Admission Infirmary Measurement and Functioning Assessment System (CAHMPAS).
- Rural Quality Improvement Technical Assistance (RQITA) – Seeks to improve healthcare quality and health outcomes in rural communities past providing information and technical assistance to State Flex Programs, Small Health Care Provider Quality Improvement grantees, CAHs, and other rural providers. Located at Stratis Health.
Where tin can I find CAH comparative information?
The Flex Monitoring Team has a number of resources that would allow y'all to criterion your CAH or find information on CAH finances and quality measures. These include:
- The Disquisitional Access Hospital Measurement and Performance Cess System (CAHMPAS) – Offers the ability to compare information on community-benefit measures at a canton and country level and quality indicators at a state level.
- CAH Financial Indicators Study: Summary of Indicator Medians by State – Provides almanac state-specific data on revenues, costs, average census, and more. The CAH Financial Indicators Primer and Calculator Resources explains how the measures are calculated and provides tools to enter your own data.
- Patients' Experiences in CAHs: HCAHPS Results, 2018 – Provides country and national averages for CAH performance on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey and state-specific reports.
- Hospital Compare Quality Measure Results for CAHs, 2018 – Offers country-specific CAH data on inpatient and outpatient quality-reporting measures from Infirmary Compare.
- Critical Access Hospital (CAH) Land Profiles – Allows users to search for state-level reports on community benefit, quality, and fiscal indicators by year.
- Community Impact and Benefit Activities of Critical Admission, Other Rural, and Urban Hospitals, 2019 – Examines the economic and healthcare benefit of Disquisitional Admission Hospitals (CAHs) on rural communities and enables State Flex Programs and CAH administrators to compare the community affect and benefit profiles of CAHs in their state to CAHs and other hospitals nationwide.
The National Rural Health Resources Center's Population Health Toolkit incorporates County Wellness Rankings, Hospital Compare, Medicare data, and Census data to help Critical Access Hospitals (CAHs), Flex Coordinators, and rural health networks employ a systems-based arroyo to motility towards population health.
If you are interested in comparing the number of beds, operating rooms, or staff, employ the HRSA Data Explorer:
- Select "Health Care Facilities" and "Cull Indicators"
- Select indicators of interest, such equally "Facility Physicians Total-Time Equivalent," and "View Information"
- Under "Facility Subcategory," type in "Disquisitional Access" and select "Contains"
For boosted quality reporting information, Medicare's Care Compare provides data on some CAHs. Yous can search by state, county, city, or zippo code to compare up to three hospitals, or download CMS Provider Information Itemize datasets.
Can a CAH own another healthcare facility?
According to Disquisitional Access Hospital Measurement and Performance Cess System (CAHMPAS) Data Summary, 60.four% of Disquisitional Access Hospitals managed Rural Health Clinics and 38.iv% provided skilled nursing care in 2018.
A survey of Critical Access Hospitals in Illinois plant CAHs are most likely to operate (versus own) dental offices, mental health practices, community health centers, retail pharmacies, and European monetary system, and were most interested in calculation customs wellness centers and behavioral health practices. The report notes CAHs may cull to collaborate with or operate other facilities rather than owning them, most often citing financial or workforce concerns.
Regarding Federally Qualified Health Centers, come across Can another healthcare organization, such as a Critical Access Infirmary, ain an FQHC? on the Federally Qualified Health Centers topic guide.
Even if a CAH does not own some other healthcare facility, information technology can also do good from collaboration and network agreements. Demonstrating Critical Admission Hospital Value: A Guide to Potential Partnerships identifies potential partners for CAHs and discusses how CAHs tin can demonstrate their value to them. A Guide for Rural Health Care Collaboration and Coordination, a publication from the Wellness Resources and Services Administration (HRSA), describes how rural organizations and facilities, including CAHs, tin develop partnerships to accost the needs of their customs. The National Rural Health Resources Center also provides a number of examples of networks that included CAHs in its Network Spotlights.
See Who can answer questions most CAH condition or reimbursement issues? for experts to contact for additional guidance on buying issues.
Can a CAH add an off-campus, provider-based clinic that does not encounter the CAH distance requirements?
As of January i, 2008, all CAHs, including Necessary Provider CAHs that create or acquire an off-campus, provider-based facility, such equally a clinic or a psychiatric or rehabilitation singled-out function unit, must come across the CAH distance requirement of a 35-mile drive to the nearest infirmary or CAH (or 15 miles in the case of mountainous terrain or secondary roads). This provision excludes Rural Wellness Clinics, equally defined under 405.2401(b), from the list of provider-based facilities that must comply with this requirement. Details nigh this requirement are available in a final rule published in the November 27, 2007 issue of the Federal Register as part of the Medicare Plan: Changes to the Hospital Outpatient Prospective Payment System and CY 2008 Payment Rates. See Section Eighteen. Changes Affecting Disquisitional Admission Hospitals (CAHs) and Hospital Conditions of Participation (CoPs), get-go on page 66877.
What are the requirements for relocating an existing CAH under the Necessary Provider replacement rules?
Critical Admission Hospitals that were granted Necessary Provider designation prior to January 1, 2006, and choose to rebuild in a new location that does not meet the current distance requirements, are treated in the same mode as if they were building a replacement facility at the original location. In guild to maintain CAH condition and the necessary provider designation, the new facility must satisfy the post-obit requirements:
- Encounter the same criteria that led to its original land designation
- Serve at to the lowest degree 75% of the aforementioned service expanse
- Offer at least 75% of the aforementioned services
- Utilize at least 75% of the aforementioned staff in its new location
See the September 7, 2007, letter from CMS to state survey agency directors titled Disquisitional Access Hospitals (CAHs): Distance from Other Providers and Relocation of CAHs with a Necessary Provider Designation for more than detailed data.
Is there a limit on the length of stay for patients at CAHs?
Disquisitional Access Hospitals must maintain an almanac average length of stay of 96 hours or less for their acute care patients. The following are not included when computing the 96-hr average:
- Time spent in the CAH as an outpatient
- Fourth dimension spent in a CAH swing bed
- Time spent in a CAH distinct office unit (DPU)
How many beds are allowed?
CAHs may have a maximum of 25 acute intendance inpatient beds. For CAHs with swing bed agreements, whatsoever of their beds can exist used for inpatient acute care or for swing bed services. Whatever hospital-blazon bed which is located in, or adjacent to, any location where the hospital bed could exist used for inpatient intendance counts toward the 25-bed limit.
Sure beds practise not count toward the 25-bed limit, including examination or procedure beds, stretchers, operating room tables, and beds in Medicare certified rehabilitation or psychiatric distinct role units. For a complete list of beds that practice non count toward the 25 bed limit, please run into Department C-0211, §485.620(a) Standard: Number of Beds: Interpretive Guidelines of the CMS Land Operations Manual: Appendix Westward.
What is a swing bed?
A swing bed is a bed that can be used for either acute care or postal service-acute care that is equivalent to skilled nursing facility (SNF) intendance. The Centers for Medicare & Medicaid Services approves CAHs, and other hospitals, to replenish swing beds, which gives the facility flexibility to meet unpredictable demands for acute intendance and SNF care.
The Rural Monitor article History of the Swing Bed: A Look Through the Rural Rearview Mirror describes the evolution of the swing bed plan to see the acute and post-acute care needs of rural residents. Swing beds offering an alternative to skilled nursing facilities. This selection may be useful in rural areas, which are less likely to have a stand up-solitary SNF. In add-on, populations in rural areas tend to exist older, and swing beds are well-adjusted for treating wellness bug typically seen in crumbling patients. The most commonly reported need was for aging patients who require rehabilitation following their hospital stay, co-ordinate to Why Use Swing Beds? Conversations with Infirmary Administrators and Staff. Furthermore, swing beds aid stabilize healthcare facilities' census and may provide financial benefits. Swing bed services in CAHs are eligible for cost-based reimbursement, while swing bed services in not-CAH pocket-size rural hospitals are paid nether the SNF prospective payment system.
For these reasons, swing bed post-astute care is mutual in rural healthcare facilities. Co-ordinate to Postal service-Astute Skilled Nursing Intendance Availability in Rural United States, 56% of all rural counties have at to the lowest degree 1 facility that provides mail-acute skilled nursing intendance through a swing bed program.
For more details most the swing bed program, see the Medicare Learning Network: Swing Bed Services fact sail and the Rural Monitor commodity Understanding the Rural Swing Bed: More than Just a Reimbursement Policy.
What emergency services are CAHs required to provide? What are staffing requirements for emergency services?
Emergency Department Services
CAHs must provide 24-hour emergency services.
Qualifying medical staff must exist onsite or on-call and available onsite within xxx minutes at all times. Onsite response times may be extended to hour if certain frontier or remote area criteria are met.
The staff onsite or on-call must meet state licensure requirements. CAH Condition of Participation: Emergency Services specifies that coverage may exist provided by a medico of medicine (Md) or doctor of osteopathy (Do), a md assistant, a nurse practitioner, or a clinical nurse specialist with experience and training in emergency care. Under temporary, limited circumstances, coverage may be provided past a registered nurse. In a June 7, 2013, memorandum, CMS clarified these requirements past stating that under CAH CoPs, an MD or Exercise is not required to be available in addition to a non-physician practitioner. Additionally, this requirement may be met in whole or in office through the use of an MD or Practice via telemedicine.
As of October 1, 2007, CMS requires that any hospital, including a CAH, that does not accept a physician on site 24 hours per day, 7 days per calendar week, provide a detect to all patients upon admission. The notice must accost how emergency services are provided when a doctor is not onsite. For more than information, delight meet page 47413 of the Baronial 22, 2007, Federal Register notice, Medicare Program; Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates; Concluding Rule.
Emergency Medical Services
Unlike emergency department services, CAHs are not required to provide emergency medical services.
Characteristics and Challenges of Rural Ambulance Agencies – A Brief Review and Policy Considerations notes that dissimilar Critical Admission Hospitals, ambulance services are typically non reimbursed at-cost. As a issue, many CAHs are not inclined to maintain an ambulance service. According to Community Impact and Benefit Activities of CAHs, Other Rural, and Urban Hospitals, 2019, 21.viii% of Critical Access Hospitals provided ambulance services in 2019. Nonetheless, after accounting for the part of hospital health systems and articulation ventures, 52.4% of CAHs had access to ambulance services. In addition, 47% of CAHs were designated as certified trauma centers.
The Frontier Community Health Integration Project (FCHIP) Sit-in, a joint demonstration project between the Centers for Medicare & Medicaid Services and the Federal Office of Rural Health Policy, reimbursed ii participating CAHs 101% of reasonable costs of furnishing Medicare Part B ambulance services instead of being paid under the Medicare ambulance fee schedule. These CAHs utilized the funding to provide increased stipends to volunteer emergency medical technicians (EMTs), hold additional EMT preparation classes, and purchase equipment. Although FCHIP initially concluded in 2019, the Consolidated Appropriations Act, 2021, extended the programme for an additional v years.
For more information on Emergency Medical Services in rural communities, see RHIhub'southward Rural Emergency Medical Services (EMS) and Trauma topic guide.
What kinds of agreements does a CAH need to have with an acute care infirmary?
As part of the agreements provision in the CAH Conditions of Participation, a CAH must develop agreements with an astute care infirmary related to patient referral and transfer, advice, and emergency and non-emergency patient transportation. The agreement must include at least ane other infirmary that furnishes astute intendance services and tin receive transfers of patients requiring services that are not available in the CAH.
The CAH may also accept an agreement with its referral hospital for quality assurance, or choose to take that agreement with some other system. State networking requirements vary. For more information on quality balls options, see What are the quality assurance and quality comeback options for CAHs?
Where tin I find examples of CAH network agreements, tools, and other materials?
RHIhub's Resource by Topic: Critical Access Hospitals lists hundreds of resource from organizations beyond the country. You tin narrow the list past selecting resource type "Tool" for a number of financial and quality tools specific to CAHs.
The Arizona Disquisitional Access Hospital Designation Transmission provides samples of a:
- Rural Wellness Network Understanding (p. 23-27)
- Rural EMS Agreement (p. 28)
- Community Needs Assessment Template (p.31-33)
How practise staffing and other requirements for CAHs differ from those of full general acute intendance hospitals?
Nether the Medicare Conditions of Participation (CoP), CAHs are granted greater staffing flexibility through two main provisions:
- Medical Staff
A Disquisitional Access Hospital must take at least one MD or DO md, but that person is non required to exist onsite. Advanced practise providers, such as physician assistants, nurse practitioners, and clinical nurse specialists tin be an independent part of the medical staff and can provide direct service to patients, including emergency services. - Nursing Staff
General acute intendance hospitals are required to accept a registered nurse onsite 24/7. Federal requirements allow for CAHs to close, and therefore have no nursing staff on duty, if the facility is without inpatients. Boosted requirements vary past state. For example, some states may offering flexibility past allowing an LPN to comprehend a shift in place of an RN when at that place are no acute patients. Contact your state survey agency for details.
CAHs must continue to come across their state licensure laws if those are stricter than the Medicare CoP.
Aside from staffing differences, requirements for CAHs and general acute intendance hospitals are very similar. CAHs must meet the requirements for the services they choose to provide. For example, if a CAH provides surgical services, it must encounter the same relevant surgery requirements as a general acute care infirmary.
Some issues may vary from state to state based on state licensure laws or other factors. To find out more virtually your state's requirements, contact your State Rural Hospital Flexibility Program Contact.
Are Disquisitional Access Hospitals eligible for the 340B program?
The 340B programme allows certain eligible healthcare facilities to buy prescription and non-prescription medications at reduced price. Critical Access Hospitals that come across the eligibility criteria are able to participate in the 340B program as a Covered Entity. A 2018 written report from the Government Accountability Office indicated that 77% of all CAHs participated in the 340B program in 2016 and accounted for 45% of all hospitals participating in the programme that twelvemonth.
See RHIhub's Rural Pharmacy and Prescription Drugs topic guide for more than information near the 340B programme.
What sources of capital funding be for CAHs?
Critical Access Hospitals (CAHs) qualify for a variety of capital letter funding opportunities, such equally grants and loans. Among others, the following two federal programs focus on helping CAHs with their capital funding needs:
- USDA Customs Facilities Loan and Grant Programme – Provides funding to construct, expand, or improve rural healthcare facilities, including CAHs.
- HUD Department 242: Infirmary Mortgage Insurance Program – Helps rural healthcare facilities finance new construction, refinance debt, or buy new equipment such as hospital beds and function machines.
Visit the funding section of this guide and the Capital Funding topic guide for additional opportunities and information.
What is the CAH survey process?
A facility interested in CAH condition should contact its state survey agency to request application materials. The country agency will review and forward the application to a CMS regional office. The CMS regional office will authorize a survey, and the state bureau will then contact the facility to adjust a survey date. The survey will verify that the CAH meets the federal facility requirements. Details about the survey procedure are bachelor in Appendix W of the CMS Land Operations Manual.
A facility volition also need to exist recertified by the state survey agency on a schedule consequent with the survey guidelines issued past CMS each twelvemonth. A facility may exist decertified if a state of affairs or issue presents firsthand jeopardy and is not resolved rapidly. Details nearly the recertification procedure are in Chapter 2 of the CMS Land Operations Manual.
Additionally, facilities may obtain deemed condition if accredited past a CMS-approved Medicare accreditation organization. In the instance of a deemed provider, the state bureau does non conduct an initial survey. While the facility seeking deemed condition must still contact the state agency to acquire the Medicare and/or Medicaid certification materials, initial certification and subsequent recertification is performed by the accrediting organization. CMS maintains a list of Approved Accreditation System Contacts for Prospective Clients. The following accreditation organizations are approved for CAH certification:
- DNV GL – Healthcare (DNV GL)
- The Joint Commission (TJC)
What legislation has afflicted the Disquisitional Access Hospital plan?
Co-ordinate to the American Infirmary Association, several pieces of legislation have modified the Critical Access Hospital (CAH) program since its creation through the Balanced Upkeep Act of 1997. The post-obit legislation are integral to the Disquisitional Access Infirmary (CAH) program:
- Counterbalanced Budget Act (BBA) of 1997
Created the CAH program, outlining all details of the program including eligibility and operational regulations. - Medicare, Medicaid, and SCHIP Counterbalanced Upkeep Refinement Act (BBRA) of 1999
Corrected unanticipated adverse payment and regulatory consequences of the BBA of 1997. - Medicare, Medicaid, and SCHIP Benefits Improvement and Protection Act (BIPA) of 2000
Provided further exemptions and reimbursement improvements to CAHs, which strengthen the overall program. - Medicare Prescription Drug, Improvement, and Modernization Act (MMA) of 2003
Enhanced CAH payments, expanded bed-size flexibility, provided continued funding for the Medicare Rural Hospital Flexibility (Flex) Programme grants, and increased Medicare payments to 101% of reasonable costs. It also enacted a sunset of the necessary provider provision, effective January 1, 2006. - Medicare Improvements for Patients and Providers Human activity (MIPPA) of 2008
Further expanded Flex grants, and allowed CAHs to receive 101% of reasonable costs for clinical lab services provided to Medicare beneficiaries even if the specimen was collected offsite or at another CAH-operated facility. - American Recovery and Reinvestment Human activity (ARRA) of 2009
Created several grant, loan, and incentive programs to back up the adoption of new wellness information technology (Striking) in CAHs. - Patient Protection and Affordable Care Act (ACA)
Included several efforts aimed at reducing workforce shortages, such every bit expanding Area Health Didactics Centers (AHECs) and further investing in the National Health Service Corps. It too immune CAHs to participate in the 340B program, making reduced cost pharmaceuticals accessible in rural communities. - Budget Control Act of 2011
Imposed mandatory across-the-board reductions in federal spending to achieve $1.2 trillion in budget savings over a 10-twelvemonth menstruum (also known as sequestration). - Bipartisan Budget Act of 2013/Pathway for SGR Reform Act of 2013
Extended sequestration for an additional two years (2022 and 2023) beyond the catamenia specified in the Budget Control Act of 2011 at the same percentage of spending. The Bipartisan Upkeep Acts of 2015 and 2018 extended sequestration through 2027. The Coronavirus Assistance, Relief, and Economical Security (CARES) Deed further extended sequestration through fiscal year 2030. However, the CARES Act besides paused sequestration amid the COVID-19 pandemic, and legislation passed in April 2021 extended the suspension through December 2021.
RHIhub'due south Rural Wellness Policy guide provides additional information on policies and legislation affecting rural healthcare.
What are Rural Emergency Hospitals?
The United States Congress established the Rural Emergency Hospital (REH) every bit a new Medicare provider blazon in the Consolidated Appropriations Act, 2021. Effective January one, 2023, this law volition allow Critical Admission Hospitals and other pocket-size rural hospitals meeting eligibility criteria to convert to Rural Emergency Hospital (REH) status. REHs will be reimbursed at 105% of the outpatient prospective payment system (OPPS) for emergency and outpatient care services in add-on to a stock-still monthly payment. Unlike Critical Access Hospitals, REHs will not be allowed to provide inpatient services.
See RHIhub'southward Rural Hospitals topic guide for additional information on Rural Emergency Hospitals.
Your State Rural Hospital Flexibility Program Contact tin can provide ongoing guidance nigh CAH bug. Other important contacts include:
- CMS Regional Function Rural Health Coordinator – for questions about CMS regulations
- State Survey Agency – for survey and certification questions
- National Rural Health Resources Center's Technical Assistance and Services Center (TASC) – for technical aid, information, and other resources
- Medicare Administrative Contractor (MAC) – for questions nigh Medicare claims, reimbursement, and billing issues

Which Of The Following Is Not True Regarding Hospital Emergency Services.,
Source: https://www.ruralhealthinfo.org/topics/critical-access-hospitals
Posted by: pridgentwitir.blogspot.com
0 Response to "Which Of The Following Is Not True Regarding Hospital Emergency Services."
Post a Comment